
Since the 1976-77 school year, when Congress first required public schools to count the number of children with learning disabilities (LD), the share of school-age children labeled LD has risen from 1.8 percent to 5.2 percent. Learning disabilities now account for more than half of all students enrolled in special-education programs, up from 22 percent a quarter century ago. In the past decade alone, the number of students aged 6-21 identified as learning disabled under the Individuals with Disabilities Education Act (IDEA) has increased 38 percent. The largest jump, of 44 percent, has been seen among adolescents aged 12-17–a significant yet poorly understood increase. Private and postsecondary schools have experienced similar increases.
The steadily growing number of students identified as LD invites public skepticism. Most scientific experts, however, agree that 5 percent, and likely more, of our school population suffer severe difficulties with language and other skills. Even so, the disproportionate rise in the incidence of LD, especially among adolescents, does raise questions about the methods of identifying and treating learning disabilities.
What explains the rise of LD? Is it the result of positive developments, such as improved identification methods? Or is the definition of LD too general and ambiguous to catch younger students before they fail? Are some students identified as LD simply the victims of poor teaching? Put another way, does the education profession adequately prepare teachers to address differences among children?
We propose that the rise in the incidence of LD is largely the result of three factors. First, remediation is rarely effective after 2nd grade. Second, measurement practices today work against identifying LD children before 2nd grade. Third, federal policy and the sociology of public education itself allow ineffective policies to continue unchecked.
The best mainstream research–studies that reflect the consensus of experts in such fields as child development, education, and neuroscience–shows that most longstanding difficulties in defining and treating LD stem from inaccurate assumptions about their causes and characteristics. Moreover, the data now justify very early identification and prevention programs for children at risk for LD. This is nowhere more true than with reading disabilities, which are by far the most common and most troublesome of these disorders, constituting 80 percent of all students with LD. Fortunately, reading disability is also the best understood and most effectively corrected learning disability. If children receive effective instruction early and intensively, they can make large gains in general academic achievement.
Early intervention can greatly reduce the number of older children who are identified as LD. Without early identification, children typically require intensive, long-term special-education programs, which have meager results. Early intervention allows ineffective remedial programs to be replaced with effective prevention while providing older students who continue to need services with enhanced instruction so they can return to the educational mainstream.
The Rise of LD
The term learning disability traditionally refers to unexpected underachievement in adequate educational settings. Students with LD do not listen, speak, read, write, or compute as well as their “potential”–usually as measured by IQ—suggests they should. Historically, neurobiological factors–put crudely, glitches in the brain–were blamed.
Conditions resembling unexpected underachievement are found in medical and psychological literature beginning in the mid-19th century, where they are described variously as word blindness, dyslexia, dysgraphia, and dyscalculia. In 1962 Samuel Kirk, a psychologist at the University of Illinois, coined the term learning disabilities, which quickly entered professional and popular parlance. Like his more medically oriented predecessors, Kirk focused on unanticipated learning problems in a seemingly capable child. He defined LD as “a retardation, disorder, or delayed development in one or more of the processes of speech, language, reading, spelling, writing, or arithmetic resulting from a possible cerebral dysfunction and not from mental retardation, sensory deprivation, or cultural or instructional factors.” Kirk posited LD as an amalgam of disabilities, all grouped under a single label, just as the federal definition of LD has ever since. This was an intellectually bold move–but it was at best half right, and today we labor under its adverse consequences.
The term learning disability gained rapid acceptance among parents and professionals in the 1960s and ’70s. Rhetorically it exuded optimism. It did not stigmatize children; it imputed no shortage of intelligence, no emotional disturbance, no troubled home life, no bad schools. It almost presumed cultural and environmental advantage. Pragmatically it spoke to a real problem: before the 1960s, underachieving children couldn’t receive special education unless they were mentally deficient, emotionally disturbed, or physically handicapped. Professional and parental advocacy soon led to the 1969 Learning Disabilities Act, followed by the 1975 Education for All Handicapped Children Act (renamed the Individuals with Disabilities Education Act in 1990).
Most definitions of LD have at least four elements in common. The four elements posit LD as: 1) heterogeneous; 2) intrinsic or neurobiological; 3) marked by a significant discrepancy between learning potential (measured intelligence) and academic performance (measured skills in reading, writing, mathematics, and oral language); and 4) not caused by cultural, educational, environmental, or economic factors or by other disabilities (such as mental deficiency, visual or hearing impairments, or emotional disturbance).
The tenacity of these elements in definitions of LD has grounded our public policies and pedagogy in outdated science and flawed understandings of the nature of these disabilities. Their validity is rarely scrutinized, and the results of these occasional examinations are typically ignored. We suspect this impasse owes not to the evidence as much as to professional and political inertia.
New Definitions
In federal legislation, LD is not a single disability but a category of special education composed of disabilities in any one or more of seven skill domains: listening, speaking, basic reading (decoding and word recognition), reading comprehension, writing, arithmetic calculation, and mathematics reasoning. These disabilities can be accompanied by emotional, social, and behavioral disorders, including attention deficits, but they cannot, in the federal definition, be the primary cause of the learning disabilities.
If the current policy definition of LD creates a deliberately wide net, with seven possible disabilities, it also invites sloppy science. The definition tells us only what LD is not. This has provoked recent calls for changing the various domain-specific categories to reflect evidence-based research and to specify criteria for identifying the attributes of different learning disabilities. This recommendation is based on the observation that generic definitions, while useful for political, advocacy, and compliance purposes, get in the way of good practice in identifying and teaching students with LD and conducting research. To date this recommendation has made little headway in entrenched special-education communities; it failed to find its way into the 1997 reauthorization of IDEA. Until this bold but elementary initiative is undertaken, the assessment and instruction of children with LD will remain unreliable.
New evidence on neurobiological causes. The study of learning disabilities was founded on the assumption that neurobiological factors were the basis of the problems with learning. Neurobiological dysfunction was inferred from what was known about the linguistic, cognitive, academic, and behavioral characteristics of adults with brain injuries, as well as from evidence that reading problems run in families. Until recently, explanations of LD continued to favor neurobiological (or intrinsic) rather than environmental (or extrinsic) causes.
New, objective ways to assess putative brain dysfunction have led to extraordinary breakthroughs, especially in the area of reading. A sizable body of evidence indicates that poor readers exhibit disruption primarily, but not exclusively, in the neural circuitry of the brain’s left hemisphere, the part that serves language. Investigations using post-mortem brain specimens and magnetic resonance imaging (MRI) suggest subtle structural differences in several brain regions between reading-disabled (RD) and nonimpaired readers. More significant is the converging evidence from studies based on functional brain imaging that reveals the activity of the brain while someone reads. These studies indicate a pattern of brain organization
in poor readers that differs from that seen in nonimpaired readers, with less activity in regions of the left hemisphere that are associated with proficient reading.
Functional brain imaging, conducted while a child reads words, is also being used to show how intensive teaching can influence the brain’s reading circuitry (see Figure 1). Imaging occurs before and after intervention, during which children significantly improve in reading ability. It appears that after intervention, brain activation patterns shift to the normative profile seen in nonimpaired readers. This finding, if it can be replicated, appears to show that the neural systems supporting reading develop during interaction with the environment, including instruction.
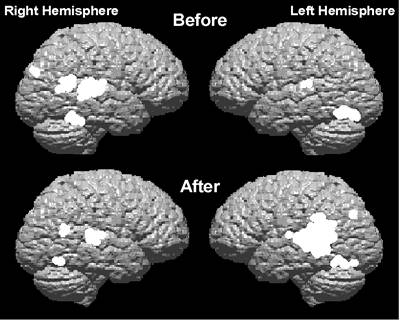 |
| Figure 1-Neural systems supporting reading may not be fixed, but develop if challenged. Shown is an image of a 10-year-old with severe reading disabilities before and after 60 hours of intensive instruction, during which the child rose into the average range in word-reading ability. The “before” image captures a brain exhibiting the standard activity pattern of children with reading disabilities. The “after” image shows increased activity in the left hemisphere, a pattern common to nonimpaired readers.
|
Genetic studies of the reading disabled reinforce this interaction perspective. Reading problems have long been known to recur across family generations; an offspring of a parent with RD is eight times more likely to have a reading disability. Studies of twins strongly support the genetic link to LD, pointing to regions on chromosomes 1, 2, 6, and 15. However, genetic factors explain only about half of the variation in reading development; environmental factors account for the other half.
This finding suggests that what is inherited is a susceptibility to RD that the environment can trigger. For example, parents who read poorly may be less likely to read to their children. In such cases, high-quality reading instruction in school is critical, as confirmed by recent studies of identical and fraternal twins. Scientists at the University of Colorado led by psychologist Richard K. Olson have explored the relationship between IQ levels and genetic and environmental influences on RD. They found that genetic influences tend to be more important for children with RD who exhibit relatively high IQ scores, while environmental influences tend to be more important for children with RD who possess relatively low IQ scores. The researchers argued strongly against excluding such relatively low IQ children from intervention simply because there wasn’t a great discrepancy between IQ and achievement. It is a grim fact that the traditional requirement of a discrepancy winds up excluding children who most need help.
Discrepancy between ability and achievement. Not surprisingly, the discrepancy criterion has proved contentious. This criterion was federally recommended in the wake of the 1975 Education for All Handicapped Children Act, which called for “objectively and accurately” distinguishing the child with learning disabilities from children with other academic deficiencies.
The use of a discrepancy between aptitude and achievement to “objectively determine” the presence of LD probably seemed reasonable at the time. Long before severe discrepancy became synonymous with LD, practitioners puzzled over the inability of some children of average and superior intelligence to master academic concepts. The discrepancy metric also reflected the common but incorrect view that IQ scores were robust predictors of an individual’s ability to learn. Despite the admonition of Edward L. Thorndike and others that IQ scores primarily estimate current cognitive functioning and not learning potential, in 1977 policymakers recommended using the scores inappropriately, as they have ever since.
These false assumptions about IQ and learning potential lead to unreliable formulas for discerning discrepancies themselves. As has been widely documented, the formulas are so fraught with psychometric, statistical, and conceptual problems that they are often useless. The discrepancy metric may even harm more children than it helps, as when the formulas used by different states deprive some students of special education following a family’s move from one state to another. Even worse, the entire measurement practice interferes with the early identification of LD. Children must fall below a predicted level of performance before becoming eligible for special education. Yet such underperformance cannot be measured reliably until a child reaches about nine years of age, or the 3rd grade. However, epidemiological data show that most children who read poorly at age nine or younger read poorly as adults. The IQ/achievement-discrepancy method creates a “wait-to-fail” model: we wait until they fail.
Another flaw in using the discrepancy concept is the inequitable education that results. No converging evidence shows an intrinsic “processing” difference among students who are weak in reading, whether they exhibit a discrepancy or not. Likewise, no evidence shows a difference in the effect of intensive instruction. The discrepancy requirement ultimately denies special services to garden-variety poor readers. This inequitable pattern recurs in reading disability:
Some children who achieve average scores on tests of word recognition read connected text with difficulty. Their slow reading impairs their comprehension. These readers clearly require special instruction, yet they do not receive it because reading fluency is rarely assessed. By contrast, if a slow-reading student has a high IQ, a weak word-reading score may secure him special-education services. Broadly speaking, the discrepancy formulation focuses attention on IQ and not on the reading process, irrationally favoring some individuals while allowing many deserving students to drift further and further from the education they need.
Excluding environment and other disabilities. As noted, LD by definition cannot stem from certain conditions that commonly impede learning: mental deficiency; emotional disturbance; visual or hearing impairments; inadequate teaching; and cultural, social, or economic disadvantages. This rubric makes for disastrous policy as well. First, it adds little conceptual clarity and actually constrains our understanding of learning disabilities. As the noted neuropsychiatrist Sir Michael Rutter of the University of London argues, this approach to definition suggests that if all the ordinary causes of the disorder can be excluded, the unknown–LD–can then be invoked. Second, some excluded conditions are known to impair cognitive and linguistic skills and actually lead to academic difficulties identified as LD.
An important example, too little scrutinized, is exclusion based on a student’s instructional history, no matter how incompetent. It was once thought that children who profit from instruction do not have a biologically based learning disability. However, as we have seen, brain-imaging studies of reading indicate otherwise: Instruction appears to establish the neural networks that support reading. No child is born a reader; all children in literate societies must be taught how to read.
No data exist to support the hypothesis that differences in the brain make some children respond less to intervention than other children do. The data, however, do indicate that the environment–including instruction, nutrition, prenatal and postnatal care, and parental drug abuse–influences neural development for better or worse. Children thus affected need the best instruction at the earliest possible time, but current federal definitions of LD preclude such a basic, sensible policy. Studies show that programs like Head Start, which are designed to prepare children for school, do a poor job of getting children ready to read. The largest federal study to date found that, on average, children left Head Start knowing only one letter of the alphabet, and that many teachers were discouraged from teaching the alphabet. Yet alphabetic knowledge in kindergarten is the single best predictor of reading success.
Preventive Education
Proficient young readers are phonemically aware, understand how print represents the sounds of speech, can apply phonemics and phonics rapidly and fluently, and connect their reading to their background knowledge. Poor readers enter kindergarten lacking phonological awareness and word-reading skills. Their text reading is laborious, impeding their comprehension and robbing them of the enjoyment of learning. Frustration and loss of interest in reading follow, as do mounting weakness in vocabulary and trouble in other academic subjects. And the cycle goes on.
Therefore, we must intervene as early as possible in a child’s school career to avoid the reading failure that will otherwise occur. Since the causes of most early reading difficulties are similar regardless of whether a poor reader meets the aptitude/achievement-discrepancy definition of LD, it makes no sense to wait for a discrepancy to reveal itself.
The tragic likelihood of failure, in the absence of very early intervention, is confirmed in numerous studies. As noted earlier, children identified as reading disabled after 2nd grade rarely catch up to their peers. Figure 2 shows the development of reading skills from the Connecticut Longitudinal Study directed by Yale University pediatrician Sally E. Shaywitz, which followed children from kindergarten through grade 12. Three groups were traced: 1) unimpaired children; 2) children defined in 3rd grade as RD due to an aptitude/achievement discrepancy; and 3) those so defined simply by low achievement. The pattern is growth from age 6 to age 12, then a near plateau from age 12 to 18. Children in the two RD groups show similar growth; neither group catches up to the skilled readers, even though half the children were pegged for special education. More than 70 percent of children identified as RD in 3rd grade remain RD in 12th grade. This longitudinal study shows that children fall behind in reading long before 3rd grade. Fortunately, other studies show that such children can be reliably identified well before 2nd grade. Researchers have found a strong relationship between phonological awareness and word recognition in kindergarten and 1st grade on the one hand and reading proficiency at the end of 4th and 5th grades on the other.
Early intervention is especially warranted given the documented failure of remediation through conventional special education. In a revealing analysis of a large data set, Hoover Institution economist Eric Hanushek and his colleagues found that placement in special education in grades 3-6 was associated with gains of 0.04 standard deviation in reading and 0.11 in math; such small gains indicate that children with LD clearly are not closing the gap. Remediation for older children fails for several reasons, but two stand out. First, quality: the instruction is frequently skimpy, highly general, and unsystematic. Second, timing: even excellent instruction may come too late, since many children lose their motivation to learn to read after a year or more of failure.
A group led by Florida State University professor of psychology Joseph K. Torgesen assigned severely disabled readers in grades 3-5 to one of two remediation programs, where they received 67.5 hours of individualized instruction over an eight-week period. Figure 3 describes the children’s growth in word reading and reading comprehension during the 16 months they were in special education before the research intervention (pretest to pretest). It also describes their growth during intervention (pretest to posttest) and in the two years following. The children showed little change in the 16 months of special education but made major improvements after a stronger intervention and maintained their gains for two years afterward.
Although these results show that older children can be substantially helped by intensive teaching, many of them remained very slow readers, with scores two years later on measures of reading fluency that were below the 5th percentile. In accounting for these mixed findings, Torgesen’s group pointed out that children develop fluency by encountering more and more words through frequent reading; children who avoid reading because it is difficult accumulate enormous “practice deficits” in elementary school. After several years, they’re unlikely to catch up in the amount they have read, which is critical for improving fluency. Still, 40 percent of these children returned to general education after the intensive sessions, well above the 5 percent of special-education students who typically return.
Early Intervention
The ineffectiveness of remediation has prompted studies of prevention and early intervention, which together might reduce the number of children who eventually qualify as reading disabled or who require literacy services through federally mandated Title I programs. Prevention in the area of reading shows special promise; it has been endorsed by both the National Research Council and the National Reading Panel. Kindergartners can be identified as “at risk” for reading problems by assessing their phonemic awareness. By 1st grade, the child’s ability to read words predicts later success in reading. The National Reading Panel has identified a large body of research recommending the explicit teaching of the alphabet and phonics as part of comprehensive reading instruction programs in kindergarten and 1st grade. Comprehension and writing instruction are also important in the early grades, and they become more important as children develop accurate and fluent word recognition skills. More broadly, studies of early intervention sponsored by four federal agencies have pointed unambiguously to the effectiveness of prevention, with tantalizing evidence that it may reduce the incidence of reading disability at later ages.
The research on prevention and early intervention has its critics. Some argue that early identification is fraught with errors; they fear incorrectly labeling a student as at risk for academic failure. However, the costs of delay are too great and, besides, a label itself isn’t necessary. Ultimately all kindergarten and elementary school teachers should be trained to teach well enough so that prevention effectively occurs in the course of normal schooling. (Of course, some children will always need more help than they can get in a typical classroom.)
Other critics point to greater gains in word recognition than in reading comprehension and to diminished gains in the later grades, as in the so-called 4th-grade slump. It is important to note, however, that this slump marks a reduction in the rate of growth, not a loss of skills. The key is to teach reading throughout elementary school, increasingly integrating word reading, fluency, and comprehension.
What, finally, of the weakest learners? Such children probably require different, highly intensive, and systematic interventions over a prolonged period, with the aim of speedy improvement so they can “read to learn” in content areas. Such ideals of instruction can be realized only when, thanks to early intervention, the numbers of children with reading difficulties decline to manageable levels.
Rethinking LD
Our review of the sad state of policy and practice concerning LD leads us to recommend radical changes in three areas:
1) the definition and identification of LD; 2) teacher preparation; and 3) prevention, early intervention, and remediation.
Improving the definition of LD. First, replace the muddled, exclusionary definition of LD with evidence-based inclusionary definitions. These must specify and distinguish disabilities in reading, mathematics, written expression, and oral language. Children who need help cannot be identified reliably without domain-specific definitions.
Second, stop using IQ/achievement discrepancy as a primary marker for LD. This may require devising alternatives if they can be found to be valid. In most cases, however, student underachievement, particularly in reading, can be identified by testing skills in the academic domain in question; by direct comparisons of the student’s age and grade with speaking, reading, writing, and math skills; or simply by uneven overall performance regardless of IQ level. IQ is an unnecessary and distracting component of the ways in which we think about learning disability.
Third, admit environmental influences into consideration. Government policies exclude inadequate instruction, cultural and social factors, and emotional disturbance, because there are other categories in special education or other services for these children, not because their academic difficulties are different or because these excluded children need different types of interventions. We know that precisely these factors can hamper neural and cognitive development and place children at risk for LD.
Fourth, single out students who respond poorly even to early intervention. The complex identification criteria and expensive due process required in special education should be reserved (albeit simplified) for such children; for most others, early interventions should be made available.
One caveat: No child should be identified as learning disabled simply because of a score, without input from teachers, parents, and others responsible for the child’s education.
Improve teacher education. First, acknowledge the limitations of current teacher preparation programs. The statement that many children identified as LD are actually “teaching disabled” is unfortunately all too often accurate. Almost all children can learn to read if taught appropriately, but many miss out on the help they need because teachers are not adequately prepared. Teaching children to read is central to a teacher’s calling, but a large body of evidence shows that teachers get weak training in individual learning differences and in teaching reading to students with diverse backgrounds and abilities. Nor are teachers trained–or later encouraged–to read and apply research.
Second, do not rest hope on reforming most schools of education. There are too many reasons to doubt that change will occur any time soon, and our academically weak children are too important to wait for reform. Instead, teachers must be provided, through any means possible, with the necessary academic content, pedagogical principles, and knowledge of learner characteristics.
Third, evaluate and, if they are found effective, encourage alternative teacher preparation programs that have emerged across the country. In Texas, for example, all teachers in kindergarten and 1st and 2nd grades receive additional training in reading instruction.
Expand prevention and early-intervention programs. First, take advantage of new technology. In Texas and Virginia, teachers administer tests that help identify the instructional needs of children at risk for reading disability in kindergarten and 1st and 2nd grades. Thanks to the federal Reading Excellence Act, some states are aiming new, scientifically based reading programs at disadvantaged at-risk children. This targeting may reduce failure substantially.
Second, make prevention the work of both special and regular education, and begin early. This will mean, among other things, revising current language in the IDEA that allows states to tap children for special education based on a “developmental delay” only between the ages of 6 and 9. In this and many other instances, complicated federal mandates for determining eligibility tend to suck up precious funds, where a few simple criteria would reap greater benefits for children.
Third, make special education accountable for the results of these interventions. Current federal policy produces a focus on eligibility and compliance that creates a labyrinth of paperwork for schools, teachers, and parents. Let’s focus instead on results, on whether the child learns to read or do math!
If these recommendations succeed, the meaning of LD could change. The label “LD” would be reserved for children whose reading or other academic problems proved severe and intractable. They would receive more comprehensive and intensive help faster. In turn, they would prompt researchers to more focused study, accelerating understanding of how the environment, the brain, and heredity interact to mold cognitive competencies. This is by no means an attempt to write off children who do not respond to aggressive instruction; it is an attempt to maximize their learning potential through scientifically sound practice. The linkage between science and policy on learning disabilities has been fragile for more than 30 years. Policy has driven the scientific agenda. This should be reversed. Learning disabilities are not that mysterious. The best consensus research, especially in the past 15 years, has profound implications for understanding learning disabilities and contradicts current policy. Clear, convergent findings are only the first step, however. A radical restructuring will succeed only if educators acknowledge the complexity of the task.
—G. Reid Lyon is a research psychologist and chief of the Child Development and Behavior Branch of the National Institute of Child Health and Human Development at the National Institutes of Health. Jack M. Fletcher is a neuropsychologist and professor of pediatrics and the associate director of the Center for Academic and Reading Skills at the University of Texas-Houston Health Science Center. To view their essay in its entirety, log on to www.edmattersmore.org.